
October 7, 2020

America’s Frayed Safety Net Undermines Improved Primary Care
Key Takeaways
- Many high-cost Medicare and Medicaid patients suffer from multiple chronic conditions that have been poorly treated or left untreated, often for many decades.
- The healthcare system does a poor job in addressing their longstanding mental and behavioral health issues, and, until recently, never sought to address their underlying need for housing, food, clothing and transportation assistance.
- Now that some providers are seeking to provide that assistance, they’re running up against the fact the U.S. has the least generous social safety net among all advanced industrial nations.
- Under the best of circumstances, it is unrealistic to think healthcare providers can make up for the inadequacy of government programs.
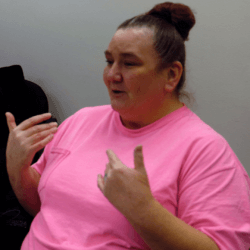
On the day caucus-goers flocked to high school auditoriums across Des Moines, 52-year-old Catherine Gothard, a recovering alcoholic and drug addict, began preparing for a job interview at a local restaurant. Her first stop was a visit to CareMore Health’s primary care clinic to pick up a decent pair of shoes from its used clothing closet.
“They have always been here for me. They have never judged me,” she said. “I’ve come here all strung out and they are always here for me.”
Gothard’s journey with CareMore began over three years ago when a stranger called her at her pizza parlor job to invite her in for a primary care visit. It was CareMore’s outreach worker, whose job was to schedule appointments for the most expensive patients among the 8,000 Medicaid beneficiaries assigned to CareMore under Iowa’s new Medicaid managed care program.
“It was weird. Here was someone reaching out to me,” she recalled. “I said okay. I think this might be a good thing for me.”
Gothard has spent three decades on and off Medicaid. She used the city’s public hospital for emergencies and its walk-in clinics for pediatric care for her three children, now grown. She grew up with an abusive, alcoholic and addicted father (“He should have never had girls; he shot up heroin in front of me.”) and spent most of her adult life with an abusive husband. Both were addicted to drugs and alcohol. She moved in and out of jails, rehab facilities and halfway houses. “The only time I was sober was when I was pregnant,” she said.
Gothard has repeated that pattern under CareMore, despite its having devoted substantial resources to her rehabilitation. Her primary care physician assigned her to a psychiatric counselor who diagnosed her with post-traumatic stress disorder, mood swings and anxiety. She enrolled in an inpatient detoxification program at a local behavioral health center. She began taking medications for her anxiety and hallucinations. Yet she relapsed, fell into a deep depression, and wound up overdosing three times, landing her in a local hospital’s ICU each time.
In the past year, she’s also been diagnosed with high blood pressure and diabetes. Her knees are giving out after decades on her feet in near-minimum wage restaurant jobs. But when I met her, she’d been sober for nearly two months while living at a halfway house, and was ready for a new job that will allow her to live on her own rather than return to her adult son’s couch. “I’m full of hope,” she said.
Her social worker at CareMore, Theresa Walker, is worried, though. “She’s going to be making $12 an hour,” she said. “There’s never enough places for people to live. It’s hard to find some place on that level of wages.” Moreover, if she earns over $25,000 a year, she’ll get thrown off Medicaid, even though Iowa expanded coverage under the Affordable Care Act. The new job – if she lands it – doesn’t provide health insurance.

Organizations like CareMore believe team-based primary care that links patients to support services in the community can substantially reduce healthcare costs and produce better outcomes. They’re taking on the most difficult challenge in modern medicine – caring for the sickest and poorest among the 5% of patients in Medicaid and Medicare that account for about half of all program costs.
But even a cursory examination of these patients’ lives reveals they are often victims of a lifetime of mental and physical abuse. They reenact behavior patterns that have run in their families for generations. Gothard said her grandfather used to beat her grandmother.
Many suffer from substance abuse and behavioral health disorders. They frequently develop multiple chronic conditions from their obesity, smoking and decades of working at menial jobs that do not provide enough money for decent food and shelter. Many go through temporary bouts of homelessness or find themselves living with relatives as they try to get themselves into a more stable situation.
In many advanced industrial countries, the government steps in to provide a safety net for people living out their lives on the lowest rungs of the economy. But other countries are far more generous than the U.S. They set a higher floor on wages. They provide larger government pensions. Healthcare access is universal and doesn’t depend on the benefits provided by employers. Their food and housing subsidies are more comprehensive.
The Organization of Economic Cooperation and Development (OECD) maintains a database that compares the relative level of income support and social service spending among its 38 member nations. The membership includes large swaths of Latin America, Eastern Europe and the poorer countries bordering the Mediterranean. The database includes both government and private, nonprofit support.
The U.S. spends a smaller share of its gross domestic product on income subsidies for low-wage workers than all but five member countries (Japan, Chile, Korea, Mexico and Turkey are the laggards). The 1.9% of GDP the U.S. spends on wage subsidies is less than half the OECD average and a quarter of top-ranked Belgium.[1]
But where the U.S. really falls down is its spending on social services. It spends just 1.3% of GDP on social services provided by public and private programs. This does not include pensions, or healthcare, where the U.S. spends 50% more than any other country. The U.S. also relies far more heavily on nonprofit, private charities than on the government to provide those services. Top-ranked Sweden spends 7.6% on social services; it’s 3.4% in Great Britain. The OECD average is 2.3%.
Our penny-pinching, pound-foolish approach to social services begins at the start of life. Although more than 72% of new mothers are full-time workers and half of two-parent families have two full-time workers, the U.S. is the only country in the OECD that doesn’t provide paid family leave for new mothers. The average OECD country provides 40 weeks.[2] Medicaid now covers 43% of new mothers in the U.S., and most of them are working.[3]
Housing is another area where the U.S. lags behind. Though we pride ourselves on being a nation of homeowners, about 35% of people rent, which is about average among industrialized countries. But a 2016 survey of a dozen advanced economies by the Joint Center for Housing Studies at Harvard University found nearly 30% of U.S. renters paid more than half their income for housing, the highest share among all the surveyed countries. Renters in the bottom fifth of income earners paid over 70% of their earnings in rent. At the same time, the U.S. subsidized just 6% of renters compared to over 50% in France, 46% in the UK and 19% in Germany.[4]
The only reason that U.S. social service spending is about equal to the OECD average is that we spend so much on direct healthcare services – now 17% of GDP. As Elizabeth Bradley and Lauren Taylor pointed out in their 2013 book, The American Health Care Paradox: Why Spending More Is Getting Us Less, “Inadequate attention to and investment in services that address the broader determinants of health is the unnamed culprit behind why the United States spends so much on healthcare but continues to lag behind in health outcomes.”[5]
Healthcare experts have long understood they must address patients’ mental and behavioral health issues if they are going to deal with the underlying problems of the poor. U.S. social conditions generate rates of mental illness and suicide significantly above other industrialized nations. Despite passage of the Mental Health Parity and Addiction Equity Act of 2008, which ostensibly requires insurers to treat mental health and addiction the same as other diseases, U.S. spending on behavioral health has fallen to 6.9% of all personal healthcare expenditures from 7.1% a decade ago.[6]
“We have 27% of the mental health professionals we need in this country,” said Andy Slavitt, the former CMS administrator who now is managing partner of Town Hall Ventures. The organization has invested in several start-ups taking on risk under Medicaid and Medicare managed care contracts. “If you look at teen mental health, there are states with only two or three pediatric psychiatrists.”
Before the COVID-19 pandemic hit, economic conditions seemed ripe for addressing these underlying issues. Jobs were plentiful. President Donald Trump triumphantly pointed to the lower unemployment and poverty rates as proof that he delivered improved conditions for low- and moderate-income Americans.
But the supposed boom times were a chimera. How many the jobs in the new service economy failed to pay a living wage?
Read Part 1: What Pandemic? Investors Love Hotspotting 2.0 to learn more.
Over 50 million or one in six Americans were still living in households with a combined income below 125% of the poverty level. That’s about what a minimum wage job pays for 40 hours a week for 50 weeks a year.
Many of the new jobs in the growing “gig” economy, now on its knees, did not provide health insurance or any other benefits. More than 2 million Americans fell into the ranks of the uninsured in the first three years of the Trump administration – before the pandemic hit – bringing the total to nearly 30 million.
Now, with an uncontrolled pandemic keeping the U.S. mired in a deep economic downturn, social conditions are growing exponentially worse. Millions of Americans are on the brink of eviction; millions more depend on Medicaid and food stamps for their basic needs.
The idea that large health systems and intensive primary care clinics can lower healthcare spending by tackling the social determinants of health has become a popular mantra among healthcare leaders. But they’re fighting an uphill battle – even in good times. Many new jobs are in low-paying service work. Housing is increasingly unaffordable for low-wage workers. The food system continues to promote obesity and disease, especially among the poor.
The U.S. social service network, meanwhile, is suffering from decades of underinvestment. It is completely inadequate to the task of dealing with poor peoples’ needs. The healthcare system does not have the capacity to treat the chronic mental and behavioral health problems, often developed over many decades, that prevent many people from succeeding at school, at work and in forming and maintaining stable families.
Can intensive primary care firms like CareMore and Oak Street Health end those cycles? “We had this hypothesis eight years ago that if you build better primary care in high acuity populations, you could lower Part A hospitalization costs and create aggregate savings,” said Dr. Griffin Myers, CEO of Oak Street Health. “It turns out it does work at the center level and at the regional level. This is a really, really big economic opportunity because if you do this well, it will pay for itself.”
But it’s not going to resolve the long-standing economic and social inequalities that in good times and in bad produce a pipeline of people in need of intensive primary care, extensive behavioral and mental health treatment. And it won’t support in meeting the basics of daily life like food, clothing and shelter.
“We don’t think about it deterministically. We have to think about it probabilistically,” Myers said. “What are the things that give us the best chance? It’s frustrating when individual people don’t have those miracles.”
Sources
- See OECD, Social Expenditure Update 2019, January 2019; https://www.oecd.org/social/soc/OECD2019-Social-Expenditure-Update.pdf.
- See Pew Research Center, Fact Tank; https://www.pewresearch.org/fact-tank/2019/12/16/u-s-lacks-mandated-paid-parentalleave/.
- Kaiser Family Foundation, Medicaid’s Role for Women, March 28, 2019; https://www.kff.org/womens-health-policy/factsheet/medicaids-role-for-women/.
- See http://www.jchs.harvard.edu/sites/default/files/brief_international_housing_carliner_marya.pdf.
- Elizabeth H. Bradley and Lauren A. Taylor, “The American Health Care Paradox: Why Spending More Is Getting Us Less,” Public Affairs, 2013, pg. 3.
- I calculated these percentages by comparing SAMHSA data on total mental health expenditures available here (https://www.statista.com/statistics/252393/total-us-expenditure-for-mental-health-services/) to total personal health consumption expenditures, available from the annual CMS expenditure reports, available here (https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/NationalHealthAccountsHistorical)

About the Author
Recent Posts

