April 26, 2016

Let’s Talk: Constructive End-of-Life Decision-Making
At Jeff Shield’s memorial service, Genie Shields proclaimed that her husband’s death has been a “gift,” one that enriches all who receive it. When it became clear that lymphoma would take his life, Jeff and Genie decided to spend his remaining time with family and friends at their rustic Flying Bear farm in southern Vermont. Jeff loved Flying Bear.
 It was summertime. Jeff “let go of the medical stuff,” lived in the moment, took walks, wrote letters, played with his grandchildren, conversed with friends, penned a memoir and reveled in the farm’s natural beauty and cycles of life.
It was summertime. Jeff “let go of the medical stuff,” lived in the moment, took walks, wrote letters, played with his grandchildren, conversed with friends, penned a memoir and reveled in the farm’s natural beauty and cycles of life.
Looking back, Genie reflects, “Jeff soared those last few weeks. As his world shrunk to just a hospital bed in the living room, the space around him just grew bigger and bigger.” The concentration of Jeff’s generous spirit into that single spot radiated outward and infected all who came near with warmth, peace and equanimity.
My wife and I became close friends with Jeff and Genie in the mid-1990s. Jeff was a leading healthcare attorney. I was a rising healthcare investment banker. We worked together on several transactions, played lousy golf and shared an interest in global affairs. As a former Peace Corps Volunteer, I was still adjusting to Wall Street’s “show me the money” culture. Jeff and Genie became important role models. They were accomplished, highly principled and flat-out cool.
In 2004, Jeff shocked many (including me) by shifting careers and repurposing himself as an academic. Jeff became Vermont Law School’s new dean and he was great at it. Dean Shields took students on weekly hikes, opined regularly on public radio, expanded the School’s premier environmental curriculum, established a U.S.-China Partnership for Environmental Law, created distance-learning and accelerated J.D. programs, undertook two major building projects and fought against the military’s “Don’t Ask Don’t Tell” policy.
Cancer cut his tenure short. At his 2012 retirement, Jeff observed,
I have loved this job. The opportunity to lead an institution with a mission of public citizenship, public service and environmental advocacy has been exhilarating. The quality and values of our trustees, faculty, staff, students and alumni have lifted me every day since I started here.
Jeff’s work wasn’t done. Acclaimed author and surgeon Atul Gawande featured Jeff in a nationally-broadcast Frontline documentary, “Being Mortal.” Camera crews trailed Jeff and Genie during his final months. After his death, Gawande confided to Genie that Jeff was the program’s “anchor.” In a last noble act, Jeff Shields provides a compelling and very public example of dying well.
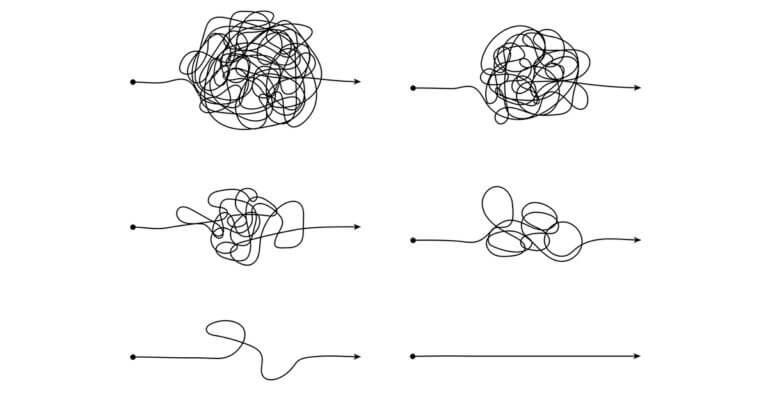
America’s Death Spiral
 Dean Nancy Kane of the Harvard School of Public Health often quips, “Americans believe death is optional.” American culture keeps death at arms-length. Americans avoid difficult conversations about death. Too often, individuals and their families confront a death spiral under duress with no preparation. They make bad decisions that cause catastrophic emotional, medical and financial consequences. Consider these realities:
Dean Nancy Kane of the Harvard School of Public Health often quips, “Americans believe death is optional.” American culture keeps death at arms-length. Americans avoid difficult conversations about death. Too often, individuals and their families confront a death spiral under duress with no preparation. They make bad decisions that cause catastrophic emotional, medical and financial consequences. Consider these realities:
- Medicare spends 26% of its funding on beneficiaries in the last year of their life.[1]
- In 2011, the average American consumed $54,017 in healthcare services during their last year of life, a 58% increase from $34,257 in 2002.[2]
- More than 90 million Americans have at least one chronic disease and 70% of Americans die from chronic disease.[3]
- Out-of-pocket expenses during the last five years of life averaged $39,000 for individuals, $51,000 for couples and up to $66,000 for people with long-term illnesses.[4]
- The percentage of Medicare patients seeing 10 or more doctors in the last 6 months of their lives increased from 30.8% in 2003 to 36.1% in 2007.[5]
- Medical expenses account for 62% of personal bankruptcies in the U.S. In 72% of these bankruptcies, individuals had health insurance.”[6]
- 70% of Americans would prefer to die at home.[7] Instead 70% die in hospitals, nursing homes or long-term care facilities.[8]
- “More than 80% of patients wish to avoid hospitalization and intensive care during the terminal phase of illness, but those wishes are often overridden by other factors.”[9]
- 89% of American think doctors should discuss end-of-life care with patients. Only 17% of Americans have discussed end-of-life care preferences with physicians.[10]
The majority of Americans do not receive end-of-life care consistent with their values and goals. Absent clear direction, the American medical system adopts an “all necessary measures” approach that generates excessive treatment, high costs and reduced life quality. Rather than end life on their own terms, patients die overburdened in institutional settings. Life’s final passage becomes a nightmare journey into oblivion. Everyone suffers.
It doesn’t have to be this way. Gunderson Health System in Lacrosse, Wisconsin is a national leader in advance care planning. Major healthcare organizations, including Kaiser Permanente and Dartmouth Hitchcock, integrate Gundersen’s Respecting Choices program into their care protocols. Applying advance care management leads to better treatment decision-making, higher patient satisfaction and lower costs. Gundersen’s cost during the last two years of life is 28% lower than Wisconsin statewide averages.[11] When hospitals, doctors and patients work together, everybody wins.
America’s Evolving Conversation about Death
Next to a child’s birth, a good death can be life’s most powerful and human experience. People focus on what matters most. Important conversations occur. Human connection and relationships deepen. Life moves forward.
Austrian poet and novelist Rainer Maria Rilke hated how modern medicine strips dying of its “terrible intimacy.”[12] He captures the tragedy of “medicalized” death in this passage,
Love and Death are the great gifts that are given to us; mostly, they are passed unopened.
Like Jeff and Genie Shields, more Americans are choosing to receive and open the gifts a good death offers. During the last decade, multiple organizations have emerged to advance American attitudes and behaviors regarding death. They’re empowering people to undertake end-of-life care planning. They’re urging Americans to talk, learn one another’s stories and act purposefully. Let’s visit some.
Matt Holder and Alexandra Drane launched Engage with Grace in 2008 to stimulate conversations about end-of-life care. They want to ensure that people can end their lives in the same purposeful way they lived them.
 At Death Cafe events,
At Death Cafe events,
people drink tea, eat cake and discuss death. Death Cafes increase awareness of death to help people make the most of their (finite) lives.
It’s catching on. Sponsors have hosted over 2700 “death cafes” in 32 countries.
Like Death Cafe, Death Over Dinner assembles people together to discuss end-of-life planning and share a meal. Since its 2013 founding, over 70,000 people in 20 countries have attended their dinners. [13]
In 2010 journalist Ellen Goodman launched The Conversation Project “to help people talk about their wishes for end-of-life care.” Still saddened and frustrated that she didn’t know her mother’s end-of-life preferences, Goodman believes “the conversation” should “begin at the kitchen table, not in the ICU.” The Conversation Project has partnered with the Institute for Health Improvement and the Screen Actors Guild to spread the word and get people talking.
Back from the Dead to Help the Dying
 Dr. David Brown was Chair of Cleveland Clinic’s Anesthesiology Institute in 2011 when he began curative treatments for military-acquired Hepatitis C. Five months into the seven-month regimen, everything went south. Hospital-acquired sepsis led to multiple organ failure and three-plus weeks in the Clinic’s Intensive Care Unit. Periodically conscious, David felt he was watching himself die.
Dr. David Brown was Chair of Cleveland Clinic’s Anesthesiology Institute in 2011 when he began curative treatments for military-acquired Hepatitis C. Five months into the seven-month regimen, everything went south. Hospital-acquired sepsis led to multiple organ failure and three-plus weeks in the Clinic’s Intensive Care Unit. Periodically conscious, David felt he was watching himself die.
David’s family sat vigil as the days turn into weeks. Twice they discussed Do-Not-Resuscitate orders. David’s care team put him on a ventilator. Pain and delusion were constant companions. Miraculously, with “a single heartbeat,” David came back. He scrawled on his message board, “I’ve never felt so alive.”
David’s near-death experience catapulted him into a new career. He founded Curadux to help individuals and families navigate the complex and sometimes cruel medical world that treats advanced illness. According to David, “When patients lack capacity, the medical system imposes its will. If people don’t want to become a burden, they have to think about death and plan ahead.”
Curadux recommends a 5-step checklist for ensuring wise healthcare decisions:
- Assess: identify what matters most and clearly identify desired outcomes
- Explore: understand your medical condition and treatment options
- Decide: select treatment options that align with your values and goals
- Capture: formalize your decisions in written documents
- Share: communicate your decisions to family and professional advisors
David believes there are two stages to achieving a good death. The first is “Advance Care Planning” and the second is “End-of-Life Wellness.” Both are essential.
Advance Care Planning: Effective Medical, Legal and Financial Decision-Making
 Benjamin Franklin wisely observed, “By failing to prepare, you are preparing to fail.”
Benjamin Franklin wisely observed, “By failing to prepare, you are preparing to fail.”
Franklin’s wisdom applies to end-of-life care planning. The stakes are high and patients confront a “medical industrial complex” that always wants to do more; go the extra mile. Only with thoughtful, comprehensive planning can individuals and their families withstand the pressure to do more when it’s time to do less.
The best advance care planning integrates financial, legal and medical decision-making within a cohesive process tailored to individual goals and values. End-of-life care can be expensive and unpredictable. It’s essential to link investments and insurance with appropriate legal documentation. When assessing their medical risk profiles, individuals should evaluate the following:
- Likelihood of a prolonged chronic disease, such as Alzheimer’s
- The adequacy of exiting investments to cover future medical expenditures
- Strategies for minimizing tax obligations while paying for medical treatments
- The cost and relative benefits of long-term care insurance
- The availability and cost of transitioning a home into a care center
- Asset protection strategies, e.g. for individuals considering Medicaid-funded nursing home care (guidelines are state-specific)
Advance care planning integrates end-of-life treatment preferences. Engage with Grace’s “One Slide Project” challenges “individuals and their loved ones” to answer five questions:
- On a scale of 1 to 5, where would you fall on this continuum? 1 is “Let me die without medical intervention” and 5 is “Don’t give up on me no matter what, try any proven and unproven intervention possible.”
- If there were a choice would you prefer to die at home or in a hospital?
- Could a loved one correctly describe how you’d like to be treated in the case of a terminal illness?
- Is there someone you trust whom you’ve appointed to advocate on your behalf when the time is near?
- Have you completed any of the following: written a living will; appointed a healthcare power of attorney or completed an advance directive?
Talking about death doesn’t cause death. Instead, answering difficult questions about death creates a framework for end-of-life wellness. It enables individuals to design their end-of-life care plans well before they decline. This is as it should be. As the adage goes, “The best time to fix the roof is when the sun is shining.”
David Brown emphasizes the importance of establishing a durable medical power of attorney.
No checklist can cover all contingencies. Individuals need informed and trusted advocates to act on their behalf when they lack the capacity to make important medical decisions.
End-of-Life Wellness
 A satirical 1997 headline from The Onion reads, “World Death Rate Holding Steady at 100%.”[14]
A satirical 1997 headline from The Onion reads, “World Death Rate Holding Steady at 100%.”[14]
We all get older. We just die once. We don’t get to practice. We want to get it right. Getting it right requires courage to do the following:
- Accept medical realities
- Determine priorities for the time remaining
- Be pro-active in communicating personal priorities
Individuals weigh hopes (attending a wedding) and fears (not being a burden) in determining their priorities. When given the choice, most people care more about end-of-life quality than longevity.
Key decisions are whether and when to receive palliative care, sometimes called “comfort care.” Palliative care does not negate medical treatment, but shifts focus to making patients more comfortable. Interestingly, several research studies have found patients receiving palliative and hospice care live longer than patients receiving standard care.[15]
Numerous organizations offer tools to assist individuals make informed medical decisions. For example, Advance Care Planning Decisions produces short, disease-specific videos that guide patients through end-of-life care decisions. Ninety-five percent of patients viewing these video guides recommend them.
In seventeen states, individuals with terminal diagnoses can translate end-of-life care plans into actionable medical orders through POLST, Physician Orders for Life-Sustaining Treatment Paradigm. POLST emphasizes advanced care planning and shared medical decision-making (between patients and their doctors) to ensure caregivers follow pre-determined care plans.
How Doctors Die
In 2011, Ken Murray wrote an influential essay observing that doctors with terminal conditions rarely pursue extraordinary treatment measures for themselves, but do pursue extraordinary measures for their patients. Murray writes,
What’s unusual about doctors is not how much treatment they get compared to most Americans, but how little.[16]
A 2014 Stanford Medicine study confirms Murray’s observations. Almost 90% of physicians surveyed would choose do-not-resuscitate orders for themselves. This does not hold for patients. The study finds,
Doctors continue to practice aggressive treatment at the end-of-life, despite the fact that most Americans now say they would prefer to die at home without life-prolonging interventions.[17]
Each patient is unique with individual opinions regarding their care. The healthcare system should honor these opinions. What doctors always have that patients often do not is a deep understanding of their prognosis and treatment alternatives. Applying advance care planning with shared medical decision-making grants patients this knowledge.
Final Words
Many believe that sudden death in old age, free of medical intervention, constitutes a good death. That type of death is quick and painless, but also comes with no good byes and no important final conversations. The opportunity to end life on our own terms can become a profound gift for both the dying and their loved ones.
Near the end of Being Mortal, Jeff Shields speaks to the Frontline cameras a final time,
These last couple weeks, I’ve been surrounded by family and friends. It’s been terrific. Some of the best days of my life, I must say… so, I’m still a happy guy.
These were among Jeff’s very last words. He died later that day. “Death be not proud.”[18] Jeff Shields’ legacy is strong. His shining example of living and dying well endures.
The BMO Private Bank sponsored this commentary
[1] MedPAC, Spending in the Last Year of Life and the Impact of Hospice on Medicare Outlays, June 2015, p. 9
[2] Ibid.
[4] Money Magazine, Cutting the High Cost of End-of-Life Care, Penelope Wang, December 12, 2012
[5] The Dartmouth Atlas, Trends and Variations in End-of-Life Care, April 12, 2011
[6] Huffington Post, Top 10 Reasons People Go Bankrupt, May 24, 2015
[7] Time Magazine, A Kinder, Gentler Death, John Cloud, September 18, 2000
[8] Centers for Disease Control, Deaths by Place, 2005
[10] Kaiser Family Foundation, Kaiser Health Tracking Poll, September 30, 2015
[11] Gundersen Health System, Respecting Choices, Return on Investment
[12] The Atlantic Monthly, To Work is to Live Without Dying, April 1996, pages 112-118
[13] National Public Radio, Let’s Talk about Death Over Dinner, Lesley McClurg, May 8, 2015
[14] The Onion, World Death Rate Holding Steady at 100 Percent, January 22, 1997
[15]NPCO, Research Shows Patients May Live Longer with Hospice and Palliative Care, August 19, 2010
[16] Ken Murray, How Doctors Die, November 30, 2011
[17] Stanford Medicine, Most Physicians would Forgo Aggressive Treatment for Themselves at the End of Life, May 28, 2014
[18] John Donne, Sonnet X, 1609

About the Author
Recent Posts